
Audible Contrast Threshold (ACT™) Test: A Complete Guide
Description
This guide provides clinicians with a complete introduction to the Audible Contrast Threshold (ACT) test.
Table of contents
- The challenge of measuring hearing-in-noise ability
- What is ACT and how can it overcome these challenges?
- ACT research origins
- How is ACT performed?
- ACT value and hearing-aid adjustments
- Using the ACT value in a hearing aid fitting
- Putting this into clinical practice: Case studies
The challenge of measuring hearing-in-noise ability
The number one complaint reported by hearing-aid users is the ability to hear well in noisy situations. As hearing-care professionals, we need to understand the challenges our clients experience when they are in these complex listening environments and program their hearing instruments to respond appropriately. To assist us in this process, there are several tests which we use on a regular basis.
1. Pure tone audiogram (PTA)
For over 100 years, we have been using the pure tone audiogram (PTA) as our primary tool to fit a hearing aid. It defines the quantity of hearing, and we use the results to set the gain characteristics of the instrument. Although the PTA is an essential part of any audiological assessment and subsequent hearing aid fitting, it has been shown multiple times in the literature to be a poor predictor of how well a hearing-aid user will hear in noise (Killion et al., 2004). Because of this, we cannot use the PTA to help us program advanced hearing-aid features such as noise reduction and directionality and we therefore need to find other tools to assist us in doing this.
2. Speech testing in quiet
The second tool at our disposal is speech testing in quiet. These tests define the amount of speech the client has access to with and/or without their hearing aids. Speech in quiet testing gives plenty of useful information regarding the audibility of speech but again is lacking because it is a measure of hearing quantity not hearing quality. This means we must look further afield for tools to assist us with programming advanced hearing-aid features.
3. Speech-in-noise tests
Lastly, we have speech-in-noise tests. These are our true tests for measuring speech-in-noise ability. Despite being clinically available for many years (only in certain languages), these tests are not routinely performed in clinics across the world. A report by Parmar & Rajasingam, (2023) looking at the use of these tests in the UK indicates that some of the challenges associated with performing them are:
- They take a significant amount of time to run.
- These tests are language dependent – requiring validated speech materials to be created for every language.
- They often require complex equipment such as multiple speakers to produce results which replicate real world situations.
- And finally, it is not clear how we can use the results of these tests to alter the settings in the hearing aid.
It therefore becomes clear that although we have access to tools which measure the quantity of hearing, we currently struggle with finding an accessible measure that can detect the quality of hearing. This causes hearing-care professionals significant challenges when prescribing and adjusting advanced hearing-aid features. Fortunately, this has now changed with the introduction of the Audible Contrast Threshold test or ACT.
What is ACT and how can it overcome these challenges?
ACT stands for Audible Contrast Threshold. It is a test designed solely to predict a hearing-impaired person’s speech-in-noise ability. ACT is not a tone test, or a speech test. Instead, it uses modulated noise signals to determine how much ‘contrast’ a client needs to hear the difference between sounds. In other words, it estimates how well the client will hear speech in noise. The results from the test can be used to directly influence how the adaptive features of a hearing aid are programmed such as noise reduction and directionality.
ACT only takes between two to three minutes to complete and uses the same equipment as pure tone audiometry: A set of headphones (or insert earphones) and a push button. In terms of Interacoustics audiometers, you need an Affinity Compact, a Callisto™, or an Equinox Evo to perform ACT (Figure 1). Because it does not use speech material, it doesn’t matter which language the client speaks. This allows for speech‑in‑noise ability to be measured regardless of language ability.

The test is also automatically adjusted to account for the client’s hearing loss. It does this by applying the shape and level of the pure tone audiogram into the sounds they are listening to during the test. This allows for an accurate and personalized measure of speech-in-noise ability to be made.
Lastly, the results of the test can be programmed directly into the client’s hearing aid either manually or automatically, providing the hearing-aid user with an objective and personalized fitting based on their hearing‑in-noise ability.
To fully understand the ACT test and how it works, it is important to look at the research foundations supporting this test.
ACT research origins
The Interacoustics Research Unit is the research center behind the development of ACT. The ACT test is based on a psycho-acoustic measure called Spectro-Temporal Modulation (STM) detection.
STM is a test designed to present the patient with non-speech sounds which mimic the fluctuations found in speech. When describing fluctuations, think of how the amplitude of speech changes going up and down from syllable to syllable (temporal fluctuations), or how the voice goes upwards towards the end of a question (spectral fluctuations).
Another way to describe these fluctuations is to use the term modulations. The STM test uses a stimulus which imitates the modulations found in speech but instead of listening to speech, the patient listens to bursts of pink noise with these modulations imposed on top of it. When being tested, the client listens for the modulated noise bursts as they are presented among noise bursts without modulation. When modulations are present, the patient will hear them as a siren-like sound.
The concept of STM detection is that the tester starts the test at a degree of modulation where the client can clearly hear the difference between modulated and unmodulated sounds. They then reduce the degree of modulation until the client cannot differentiate it from the unmodulated sound. This is classified as the STM threshold – or the ACT value.
Early excitement in research circles
Several years ago, STM detection caused a lot of excitement in research circles because the STM threshold (the value measured by the test) has been shown to correlate closely with advanced speech-in-noise tests using a complex, multiple-speaker setup. It was thought that the results from the STM could be used to advise hearing-care professionals on how to program adaptive hearing-aid settings such as noise reduction and directional microphones. However, a study by Bernstein et al., (2016) identified that STM thresholds could only be reliably established in two out of three clients with hearing loss, indicating that modifications to the test were required to make it a clinically‑viable test.
Changes to the STM test paradigm
The Interacoustics Research Unit began their involvement with the test here. They started by making several changes to the STM test paradigm, including the development of a stimulus which would compensate and correct for the client’s hearing loss (Zaar et al., 2023a).
When these changes were made, a follow-up study was completed that showed by compensating for a client’s hearing loss, it was possible to measure the STM thresholds in all test subjects, overcoming the issue highlighted in the study by Bernstein et al, (2016). In this follow-up study, the STM thresholds were then compared against an advanced multi-speaker speech-in-noise test. It was found that the STM thresholds measured using this new method could still predict aided speech‑in‑noise scores accurately.
Related course: Audible Contrast Threshold: Introduction
Developing a clinically-friendly STM test
With this information, the Interacoustics Research Unit further developed the STM test procedure to allow it to be completed in a clinically ‑friendly way. They did this by designing the test to be used with the same equipment as standard audiometry as well as using a Hughson-Westlake bracketing technique (similar to audiometry) to determine the threshold in around two to three minutes. It was at this point where ACT was born (Zaar et al., 2023b).
Lastly, to confirm that ACT is a global test and not just a predictor for speech-in-noise thresholds in English, several studies have since been performed validating the correlation between ACT and aided speech scores in multiple languages, including Danish, German, and Japanese.
Read more: Research journey behind ACT
How is ACT performed?
As previously mentioned, ACT uses a modulated noise signal to examine speech-in-noise ability. The aim is to identify the lowest contrast level the client can detect. To perform ACT, it is mandatory for an audiogram to be completed beforehand for air conduction at the following frequencies:
- 250 Hz
- 500 Hz
- 1000 Hz
- 2000 Hz
- 4000 Hz
Inter-octave frequencies will be considered in ACT testing if they have been completed. Below, you can see a video of the test being performed in the clinic.
As you can see in the video, it is easy to perform the test, and teaching a client to complete the test is straight forward. This is because it is a similar task to pure tone audiometry. The client is asked to press the button when they identify a certain sound.
You can perform ACT with the Affinity Compact, the Callisto™, or the Equinox Evo. Follow the link below for a detailed step‑by‑step guide on how to perform the test.
Read more: How to perform the ACT test
ACT value and hearing-aid adjustments
Once an ACT test has been completed, the tester will be presented with a value. This is known as the ACT value and it is expressed in dB nCL, which stands for ‘normalized Contrast Level’. This is a novel scale developed by the research team at the Interacoustics Research Unit. In brief, nCL stands for:
- n – normalized – the scale is normalized based on normative data acquired from young adults with normal hearing. A young adult with normal hearing will thus score 0 dB nCL.
- C – Contrast – clients are detecting a contrast in terms of modulation of a signal.
- L – Level – this is a dB measure so is denoted as such. This does not refer to the presentation level but instead the amount of contrast / modulation in the signal.
The ACT value will range from minus 4 dB nCL to 16 dB nCL. It can be used to inform the hearing care professional of how well a hearing-impaired person will hear speech in background noise when wearing hearing aids. The lower the ACT value, the better the client will be able to hear speech in noise. The higher the ACT value, the more difficulty they will have hearing when in background noise.
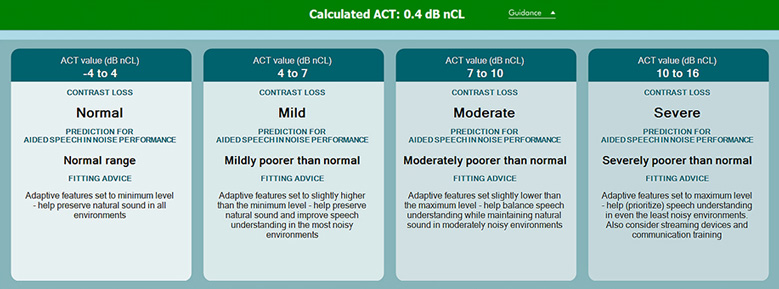
The Interacoustics Research Unit has identified normative data for the ACT values (Table 1).
| ACT value | Contrast loss |
| Minus 4 dB nCL to 4 dB nCL | Normal |
| 4 dB nCL to 7 dB nCL | Mild |
| 7 dB nCL to 10 dB nCL | Moderate |
| 10 dB nCL to 16 dB nCL | Severe |
Table 1: Normative data for the ACT values.
As the ACT value increases, the client will need more help from their adaptive hearing-aid features. In the severe range, it is also recommended that the client strongly considers remote microphone technology to improve the signal-to-noise ratio in complex listening environments.
Using the ACT value in a hearing aid fitting
Let’s now look at how you can make changes to the hearing-aid settings using the ACT value. There are two methods of doing this. The first is to automatically apply the value into the fitting software and allow the instrument itself to make the changes. The second is to manually use the value along with the counseling tool to make changes to the hearing-aid settings.
1. Automatic hearing-aid adaptive feature adjustments using ACT value
The most effective way to use the ACT value is by inputting it directly into the hearing-aid fitting software (if possible). This will optimize the adaptive features of a hearing aid automatically. Depending on the hearing-aid manufacturer, the value can be either be imported across from NOAH or there will be a dedicated area in the software where the hearing-care professional can input it. Once the value is in the software, the instrument will be automatically programmed to take the ACT value into account by changing multiple hearing-aid parameters to optimize the fitting for the client.
2. Manual adjustments to hearing-aid adaptive features using ACT value
If the hearing aid fitting software does not have an option to directly input the ACT value, then adjustments based on the ACT value can be done manually. Hearing aids usually prescribe adaptive features such as noise reduction and directionality based on the client’s audiogram as well as other data inputted to the fitting software such as questionnaires and listening preferences. The ACT value allows for a more objective method of predicting the optimal starting point for these features to activate.
Before making manual changes to the hearing device, it is important to understand how adaptive settings are programmed in the device you are fitting. Please see Figure 2 below for additional advice on the types of changes you can make based on the severity of the ACT value.
Putting this into clinical practice: Case studies
Let’s meet two individuals who arrive at a hearing-aid clinic with the same pure tone audiogram, Penny and Raul. Penny speaks English and Raul speaks Spanish. Penny and Raul have identical hearing as measured by their pure tone audiograms. You can see their audiograms below (Figures 3 and 4).
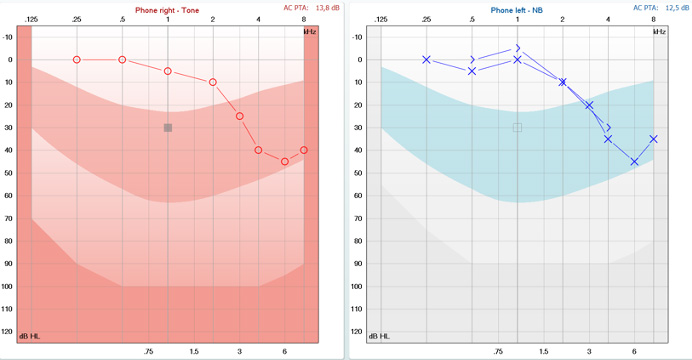
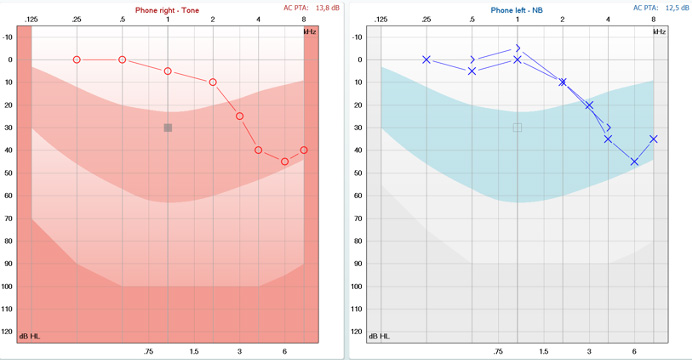
Let’s now look at their ACT values. ACT allows both individuals to be assessed using the same test despite them speaking different languages. The results from the test show that Raul has a high ACT value of 10 dB nCL. He needs lots of contrast to hear the difference in the signals. Penny on the other hand has a low ACT value of 3 dB nCL. She needs very little contrast to hear the difference in the signals.
Managing Penny
Penny has never worn hearing aids before. With the information from her PTA and ACT value, she can be prescribed some receiver‑in‑the‑ear hearing aids with a focus on retaining natural speech cues while amplifying them appropriately.
As she is going to be fitted with brand new hearing aids, the clinician can select some that incorporate the ACT value automatically. This means the hearing aids will know how best to support Penny in all situations. This doesn’t necessarily mean they should be working very hard to separate sounds more than they naturally are. We know Penny can manage this task herself quite well, as demonstrated by her low ACT value.
If she receives appropriate amplification (ensured by performing real ear measurements) to compensate for her audiometric hearing loss, then her ears and brain will be able to separate the sounds effectively. She may only need additional help from the hearing aids’ advanced features in the most challenging situations. Situations where someone with normal hearing could be expected to find it difficult too. Penny’s hearing with hearing aids should be as natural as possible so her hearing aids should be set to convey natural speech cues as much as possible.
Managing Raul
For Raul, he is an existing hearing aid user. His hearing has been well supported by his current hearing aids for quiet situations. For him, the clinician needs to try and maximize the benefit he gets from them, especially in the challenging situations. These are the situations he reported he has the most difficulty in.
His hearing aids are two years old, so not out of date or old by any means and are still appropriate for his hearing loss. They cannot automatically incorporate the ACT value, however. Raul’s hearing aids need to be adjusted manually so that the noise reduction and directionality (adaptive features) are at their maximum settings – even when the background noise is quite low.
Due to the severity of his problems with noise (as shown by his severe ACT value) he will also benefit greatly from having additional technology to hear better in noise. This could be by using a remote microphone. By understanding his ACT value, the hearing care professional can adjust the adaptive features of the hearing aids and prescribe some additional technology – meaning he can keep his current aids but get greater benefit from them.
Key takeaways
By using ACT, the hearing care professional can confidently manage clients with respect to using their hearing aids in noise. Most easily with automatic application to the hearing-aid fitting with some brands if available, but also by using the fitting and counseling guides. This is the way hearing care professionals can maximize the benefit to their clients.
Related courses
References and further reading
Bernstein, J. G., Danielsson, H., Hällgren, M., Stenfelt, S., Rönnberg, J., & Lunner, T. (2016). Spectrotemporal modulation sensitivity as a predictor of speech-reception performance in noise with hearing aids.
Killion, M. C., Niquette, P. A., Gudmundsen, G. I., Revit, L. J., & Banerjee, S. (2004). Development of a quick speech-in-noise test for measuring signal-to-noise ratio loss in normal-hearing and hearing-impaired listeners. The Journal of the Acoustical Society of America, 116(4), 2395–2405.
Laugesen, S., & Santurette, S. (2023). Audible Contrast Threshold (ACT™): A language-independent diagnostic test to quantify real-life speech-in-noise ability and personalise help-in-noise settings in hearing aids.
Parmar, B., & Rajasingam, S. (2023). Adult speech testing in the UK. ENT & Audiology News.
Vatti, M., Ratanjee-Vanmali, H., Laugesen, S., & Ghamkar, M. (2025). ACT™ in action: Enhancing client care with the Audible Contrast Threshold (ACT) test. Clinical experiences and the value of integrating the ACT test into clinical practice.
Zaar, J., Simonsen, L. B., Dau, T., & Laugesen, S. (2023a). Toward a clinically viable spectro-temporal modulation test for predicting supra-threshold speech reception in hearing-impaired listeners.
Zaar, J., Simonsen, L. B., & Laugesen, S. (2023b). A Spectro-Temporal Modulation Test for Predicting Speech Reception in Hearing-Impaired Listeners with Hearing Aids.
Presenter

