
CROS/BiCROS Hearing Aid Fitting: A Complete Guide
Description
In this article, we will equip you with everything you need to know to feel confident selecting and fitting a CROS or a BiCROS hearing aid.
Table of contents
- What is CROS?
- What is BiCROS?
- Factors to consider for asymmetrical hearing loss
- Room and patient preparation
- Hearing aid software setup
- Performing CROS fittings
- Performing BiCROS fittings
- Validation of CROS/BiCROS systems
Related course: Beyond the Basics: CROS/BiCROS
What is CROS?
CROS stands for ‘Contralateral Routing of Signal’ and CROS hearing aids are designed to help individuals with unilateral hearing loss to detect sounds from their ‘bad’ side by contralaterally routing the sound from one side to the other.
For example, if a person with single-sided deafness (SSD) were to sit in a café with a communication partner on their bad side and a noisy coffee machine on their good side, they would struggle to hear the sounds that they want to hear. By contralaterally routing the sound of their friend to the better ear, they stand a much better chance of hearing well in this situation, despite their inability to detect sound on the side that they are seated.
These systems typically consist of two hearing devices. Firstly, a standard hearing aid is fitted to the better ear with the role of presenting all the sound into the patient’s better hearing ear. A microphone is placed on the worse ear with the role of picking up sounds on the bad side and sending this sound information over to the hearing aid in the better ear to present. The hearing aid does not aim to increase the volume of sound in the good ear, but rather remain acoustically ‘transparent’.
What is BiCROS?
The Bi in BiCROS stands for bilateral, and a BiCROS hearing aid is very similar to that of a CROS, with the key difference being that a BiCROS will provide not only contralateral routing but also simultaneous amplification into the contralateral ear.
This is very useful when we are working with a bilateral hearing loss, which is also significantly asymmetrical as we are able to overcome the issue of audibility in their good ear whilst also providing bi-directional input monaurally.
As with a CROS hearing system, the BiCROS system also consists of two devices, being a standard hearing aid in the good ear and a CROS microphone in the bad side. The main difference between the two is how these devices are set up, with a BiCROS hearing aid providing significant amplification, whereas the CROS aims to maintain ‘transparency’ in the signal.
Factors to consider for asymmetrical hearing loss
Asymmetrical hearing loss can have major implications on several factors for the patient.
Cases of both unilateral hearing loss and very large hearing asymmetry can present with reduced speech performance in noise, inability to detect speakers or signals on their bad side, and elimination of binaural cues, which are important for both localization and speech in noise performance. The result of these effects can be highly distressing for individuals to manage and lead to significant reduction in quality of life.
Whilst CROS and BiCROS amplification can provide great help with many of these aspects, it is worth noting that CROS amplification will not restore these binaural cues, thus limiting the benefit for the patient in terms of localization abilities.
Distortion factors
In cases of unilateral hearing loss, one may ask:
“Why do we not just aid the poor ear?”
This may seem a reasonable question, however several factors can make this an ineffective management decision.
The first question we should ask ourselves is, will the poorer hearing ear benefit? High levels of amplification are well known to bring about a series of distortion factors which can have a significant impact upon the integrity of the signal and physiological processes within the cochlea.
Here we have an example of the hearing aid dilemma, which provides an explanation of one of the many distortion factors that we may face in hearing amplification (Figure 1).
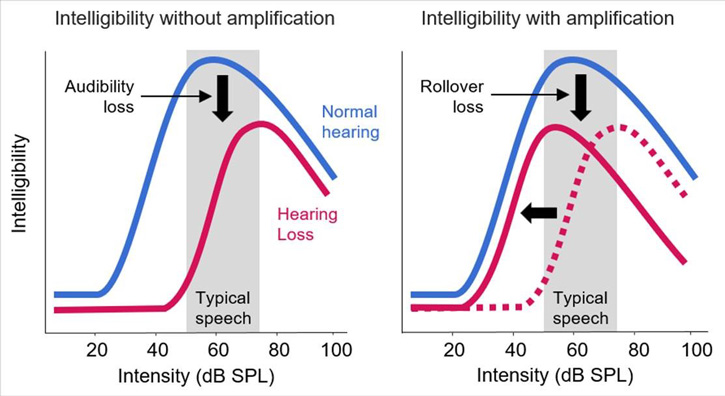
In this example, the chart on the left shows an unaided plot of speech intelligibility against sound intensity level. Note that even the normal hearing ear experiences a reduction in speech intelligibility at high intensity levels.
The aided graph on the right demonstrates that this reduction in speech intelligibility for high-intensity signals becomes even more of a factor when amplification is applied, as doing so will now effectively reduce the input intensity level at which the intelligibility reduction will become a factor.
This is commonly referred to as a ‘rollover loss’. Rollover loss is one of the many distortion factors which can occur in cases of high-intensity amplification.
Reduced dynamic range (recruitment)
Reduction in dynamic range or significant loudness recruitment can be another source of difficulty when aiding more severe hearing losses. Whilst sensorineural hearing loss reduces the audibility of low-level sounds, it does not provide a linear increase in the individual's uncomfortable loudness levels.
This can result in a reduction in the patient's overall dynamic range, leading to the need for high levels of compression or limiting. Heavy use of these hearing aid features can have an impact upon the quality of the amplified sound being delivered to the ear by introducing distortion or clipping to the output gain.
Dead regions
Cochlear dead regions are areas of the cochlea where there has been total loss of inner hair cell function. It's well established in the literature that dead regions are more common than we think, with hearing thresholds at or above 75 to 90 dB HL being the most likely to have dead regions.
This is another distortion factor which we may encounter, particularly with severe to profound levels of hearing loss. Given the increased possibility of dead regions being present with severe hearing loss, it can be sensible to consider whether the use of CROS technology might provide the patient with better sound quality by avoiding stimulating these cochlear dead regions.
You can learn more about dead regions and how to assess for them using the TEN test in the link below.
Read more: Applications of TEN Test, QuickSIN and ANL
Cross-hearing and interaural attenuation
Cross-hearing and interaural attenuation are factors which are most considered within the context of audiometry and the use of masking, but this can also be a significant factor in amplification of asymmetric hearing.
Typical transducers used for audiometry have an interaural attenuation of between 40 to 55 dB HL. Hearing aid interaural attenuation can vary significantly based upon the patient's head shape, size, and the type of hearing aid being used, however we can assume that it likely sits somewhere similar to that of an insert earphone.
With a single-sided hearing loss, it's highly likely that amplification sufficient to provide audibility in the poor ear would also be heard in the good ear. This in turn will likely introduce a degree of distortion and subsequent reduction in clarity in the good hearing ear due to the crossing over of amplification in the bad ear.
When working with one good ear, our top priority should be to maximize and preserve the good quality hearing on this side.
Significantly asymmetric hearing loss
Many of the challenges discussed above will continue to present with significantly asymmetric hearing loss, with the added challenge of the ‘good’ ear now having reduced hearing acuity.
Despite the thresholds being closer to each other, there may still be issues with limited poor-sided audibility, dynamic range, and distortion factors, as well as continued issues with potential cross-hearing.
Head-shadow effect
Another factor which we must consider with single-sided or asymmetrical hearing loss is what is commonly referred to as the head-shadow effect.
To demonstrate this effect, imagine a singing bird as the signal being listened to. As the bird sings, the sound waves it produces spread out in a roughly conical shape in front of them. The sound waves encounter the patient’s head and much of the acoustic energy is absorbed by the head.
This leaves behind an area of little acoustic energy which is referred to as the head shadow. The head shadow makes hearing a sound in an ear which is off axis to the source very challenging and is of detriment when the ear closer to the sound may not be hearing very well.
Sounds are affected to a smaller or larger extent by the head shadow based upon their frequency, with high-frequency sounds being the most impacted. The is one of the fundamental challenges which SSD or asymmetrical hearing presents.
By introducing contralateral routing of signal, we are aiming to overcome this head shadow and provide better audibility of sounds which may be blocked by the head from reaching the better hearing ear.
Alternatives to CROS/BiCROS fittings
With any intervention, you should always remain mindful of alternatives which may be present.
In some cases, a unilateral hearing loss can be adequately managed simply through the use of effective communication tactics and counseling. You should consider this based upon the patient's individual situation and the types of listening environments they are commonly finding themselves in.
Ensuring that you have open and honest communication with your patients is the best way to assess whether they need any technological intervention. Highlighting the potential pros and cons of the intervention goes a long way to helping your patients make informed decisions about how they proceed.
Bone-anchored hearing devices can also be considered for unilateral hearing loss. However, this can often be seen as being overly invasive when a CROS or a BiCROS can achieve a good result without the need for surgical intervention.
Regardless of which route you and your patient agree on, it is always important to remain aware of your patient's individual needs and preferences to guide you towards making good recommendations which are right for them.
Room and patient preparation
We can now take a look at the process involved in fitting a patient with a CROS or BiCROS hearing aid. It is important to thoroughly consider many variables when it comes to fitting these devices and we will walk through many of these below.
Equipment
You'll need access to a hearing aid fitting system such as the Affinity Compact. With this, you’ll be using a freestanding speaker and a REM headset to which you’ll be attaching a probe tube microphone. The space that you're in should be a quiet room with good acoustics, ideally a sound-treated room.
As we will discuss later, the verification process involves having your patient turn to different angles to the REM speaker and therefore having a rotating chair can be useful when getting your patient into the correct positions for the measurements.
Measurements
To allow you to move forward with the CROS, you will need your patient’s audiogram to enter into the fitting software or NOAH. It can also be helpful to undertake a middle ear assessment such as wideband tympanometry due to the significant effects that middle ear dysfunction can have upon real ear measurements.
It is important to perform otoscopy before real ear measurements to ensure that it is safe to proceed, and the ears are clear from wax or other debris.
Positioning the patient
When performing real ear measurements, it is recommended that your patient is seated approximately one meter away from the loudspeaker. You will be performing measurement at different angles, so the use of a rotating swivel chair is recommended to allow for easy movement between the measurement positions.
Protocol
If you're using the Affinity Compact, you'll find a preset protocol in the Affinity Suite for CROS and BiCROS fittings which is ready for you to use.
Read more: CROS and BiCROS fitting with the Affinity Compact
Hearing aid software setup
Once you have prepared your room and patient, the next step is to set up your device in the hearing aid software. Alison Stone, National Training Manager for Oticon UK, will demonstrate how to do this in the Genie 2 fitting software in the video below.
Performing CROS fittings
Now that you have set up the room, the patient, and the hearing aid software, you are ready to verify. We will first focus on a CROS hearing aid system, which is used to manage unilateral hearing loss. When verifying a CROS hearing aid, there are three main steps.
1. Real ear unaided response for the better ear
Run your probe tube calibration as normal, then remove the receiver hearing aid from the better ear. Place the REM headset on the patient and insert the probe tube only into the better ear.
Position the patient at 45 degrees or 90 degrees to the REM speaker with the better ear towards the speaker.
Measure the unaided response by presenting a speech signal, such as the International Speech Test Signal (ISTS), at a moderate speech level of 65 dB SPL. The obtained response will be the target for the following aided response measurement.
2. Real ear occluded response for the better ear
Through your first recording of the real ear unaided response, you have recorded the acoustic properties of the unoccluded ear canal. It's also important to consider the acoustic properties of the chosen ear tip.
To do this, perform a real ear occluded response with the hearing aid on the better ear and the patient in the same position as step 1.
In the hearing aid fitting software, run a real ear occluded response on the better ear, using the same signal you used for the unaided response. The trace should approximate the results of the unaided response.
If the real ear occluded response shows that the fitting is not truly open, you may wish to try a less occluding ear tip. If this is not possible, you may wish to consider switching from a CROS to a BiCROS fitting to help overcome some of the occlusion resulting from the hearing aid fitting.
3. Real ear aided response for the poorer ear
You have now established the acoustic characteristics of both the patient's ear canal and the hearing aid fitting. We will now move on to verify the CROS fitting with a real ear aided response measurement. However, there are a few things to keep in mind during this.
Firstly, you are going to run a real ear aided response for the poorer ear, which will verify the transparency of the CROS transmitter. Turn the patient around so that the poorer ear with the transmitter is toward the speaker.
Secondly, keep the same probe tube in the same ear as you did for the first two measurements.
Finally, perform this measurement at the same angle as the first two measurements.
Now you are ready to perform the measurement.
In the Affinity software, activate the reference microphone on the REM module on the poorer side. Measure the aided response using the same signal and level as the unaided response and the occluded response.
The obtained aided response should approximate the unaided response and occluded response for the better ear, providing a fitting that sounds transparent to the patient.
CROS adjustments
We have now seen all three steps involved in verifying a CROS hearing aid fitting. As mentioned, the aided response should approximate the unaided and occluded responses.
If the obtained real ear aided response does not approximate the unaided and occluded responses, adjust the hearing aid gain settings. This typically involves increasing gain only in the high frequencies and repeating this step.
Finally, check in with your patient that the sound quality is acceptable. Try talking to them on their good side and on their poor side, so that they can appreciate the benefit of the CROS input. You could also play some sounds through a speaker positioned on their poor side and then on their good side so they can hear the effect of transmitting environmental sounds.
Performing BiCROS fittings
The process of fitting a BiCROS aid is very similar to that of a CROS, and we will now take a closer look at his.
As we have discussed, a BiCROS fitting is a fitting designed to help with asymmetrical hearing losses, where both ears have hearing loss, but one ear is significantly better than the other. The goal of this is to overcome the head-shadow effect caused by severe hearing loss in the bad ear, whilst aiding the milder hearing loss in the better hearing ear.
Although the verification process of BiCROS is very similar to that of a CROS, there are a couple of important differences to consider. The first step involves simply fitting a hearing aid to the patient's better hearing ear using real ear measurements, as you would for any standard hearing aid fitting. Adding the BiCROS receiver to the hearing aid fitting involves two extra steps.
1. Real ear aided response for the better ear
Firstly, run a real ear aided response for the better ear, with the patient positioned at 45 or 90 degrees to the speaker, with the CROS transmitter turned off.
Secondly, turn the patient so they are positioned with their poorer ear towards the speaker. Switch on the CROS transmitter and turn off the hearing aid microphones, then run another aided response. The result of this second recording should approximate the aided response for the better ear.
2. Real ear aided response for the poorer ear
Now that you have measured the real ear aided response from the hearing aid alone, you can move on to the second measurement. For this measurement, turn the patient so that the poorer ear is facing toward the loudspeaker. As with the CROS fitting, the angle of the patient should be consistent between measurements.
The result should approximate the first aided response that you obtained for the better ear. It may deviate a little at some frequencies due to room acoustics and if an open fitting is used for the better ear.
Validation of CROS/BiCROS systems
Before discussing how to perform validation measurements with our CROS/BiCROS patients, we'll first spend a moment talking about why we should be performing validation measurements. To do this, it's important we're aligned on the differences between verification and validation.
Verification vs validation
Verification tells us if the hearing aid is working as designed whereas validation tells us if the hearing aid is working as desired. It's important you do both verification and validation as they're answering two different sets of questions, which both impact the experience of the patient (Table 1).
| Hearing aid verification | Hearing aid validation | |
| Informs whether | Hearing aid is working as designed | Hearing aid is working as desired |
| Example question | Does the performance of the hearing aid meet ANSI requirements? | Is the user satisfied with the performance of their hearing aid? |
Table 1: Hearing aid verification vs hearing aid validation.
Validation options
In this section, we will explore validation options with CROS/BiCROS patients. There are two different categories:
- Subjective outcome measures
- Aided speech testing
These are both validation measures you can perform (and combine) with these patients.
Subjective outcome measures
We'll start with reviewing our options for subjective outcome measures.
You likely have exposure to subjective outcome measures and may already be incorporating some of these into your appointments. These document the patient’s experienced benefit of using hearing aids.
COSI
There are several validated questionnaires available you can use with your patients. Something like the Client Oriented Scale of Improvement (COSI) [1] can be really beneficial because you can focus on meaningful situations specific to each patient.
You document their perception of these situations over time, and it's integrated within Noah. Since it's an open-ended questionnaire, it can lead to some nice conversations with your patients along with a better understanding of their unique needs.
APHAB
If you're looking for something more quantifiable, you can use something like the Abbreviated Profile of Hearing Aid Benefit (APHAB) [2]. APHAB has 24 situational questions broken up into four categories. You compare the unaided and aided scores to determine the benefit in these four categories.
It's a self-administered assessment, meaning it's completed by the patient, freeing up your time to perform other tasks such as servicing the patient’s hearing aids or beginning documentation.
Patient feedback
Patient feedback is also a useful form of validation. Although it doesn't necessarily give you a quantifiable score, it's still extremely valuable in the fitting and counseling process and the overall patient journey.
Also, the rapport that you'll build with authentic conversations with your patients can't necessarily be replaced with a survey.
Aided speech testing
There are several types of aided speech testing which can be useful as a validation tool for CROS or BiCROS hearing aids. We will discuss a few of these approaches below.
Aided speech reception testing
The first option we'll look at is aided speech reception testing.
First, obtain the unaided speech recognition threshold (SRT) with a loudspeaker positioned at 45- or 90-degrees azimuth related to the poor ear. Next, repeat the measurement with the CROS system on.
The difference in the aided and unaided SRT is a way of quantifying the benefit provided by the CROS system.
Aided speech perception testing
Next, we'll review aided speech perception testing.
Start by measuring the unaided speech perception score, presenting from the loudspeaker at 45- or 90-degrees azimuth relative to the poor ear. Again, we'll repeat this measurement with the CROS system on.
The difference between these unaided and aided scores is again another method of quantifying the benefit provided by the CROS system.
For this test, it's recommended to present speech at a quieter level. If the better-hearing ear in the CROS patient is normal and you present supra-threshold, it might be audible without the system.
Speech-in-noise testing
Finally, we'll look at the option of validation using speech-in-noise testing.
The first step will be to obtain an unaided signal-to-noise ratio (SNR) measurement using a validated speech test such as the QuickSIN.
To do this, you will need two loudspeakers spatially separated by 90 to 180 degrees, so placed at 45-degrees azimuth in either direction or 90-degrees azimuth in either direction.
For the unaided measurement, you will want to present speech from the speaker closer to the patient's poorer hearing ear and noise from the speaker closer to the patient's better hearing ear. For the aided measurement, you'll repeat this test with the CROS system on.
Again, you will compare the unaided and aided SNRs in this case to determine if the difference is clinically significant. To do this, you can either use normative data or your clinical judgment from your experience with CROS fittings and validation.
Related course
Beyond the Basics: CROS/BiCROS
References
[1] Dillon, H., James, A., & Ginis, J. (1997). Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. Journal of the American Academy of Audiology, 8(1), 27–43.
[2] Cox, R. M., & Alexander, G. C. (1995). The abbreviated profile of hearing aid benefit. Ear and hearing, 16(2), 176–186.
Presenter
