
Subjective visual vertical: A novel approach to otolith assessment
What is the subjective visual vertical (SVV) test?
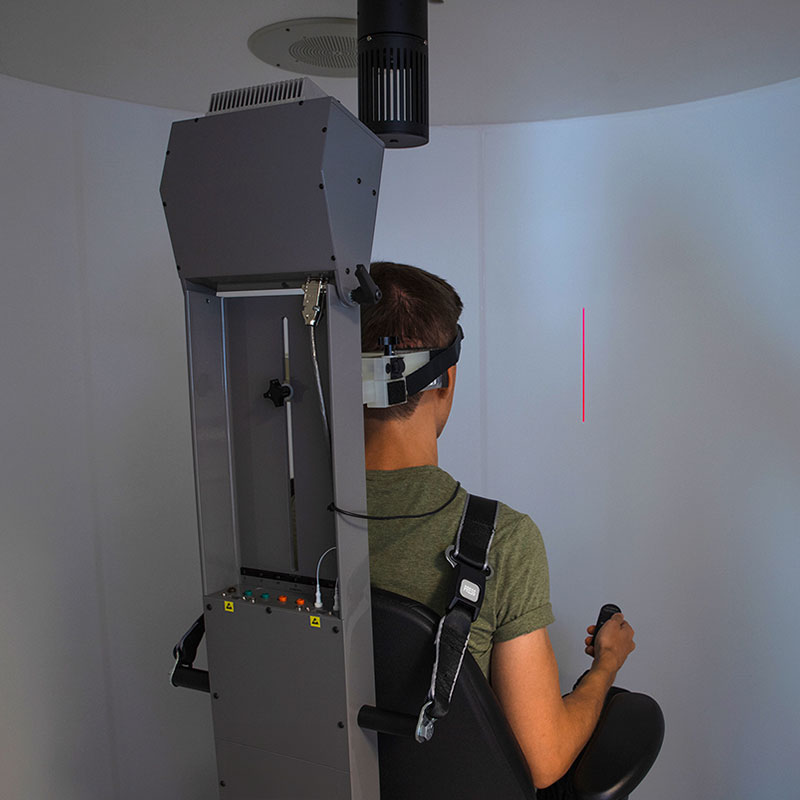
The subjective visual vertical (SVV) test is a method to test an individual's perception of verticality. In the SVV test, the patient's task is to adjust a luminous laser presented line to be parallel with true vertical in the absence of any other visual cues.
This is done in the Orion Auto-Traverse Chair (Figure 1). The sensory information required to perform this task is provided predominantly by the vestibular organs of the inner ear, and in particular, by the utricles (Clarke et al, 2003).
The roles of the vestibular organs
The vestibular organs consist of the three semicircular canals, which transduce angular acceleration, and the two otolith organs, the utricle and saccule. The otolith organs transduce linear acceleration, including gravity, with respect to the head. Of critical importance, the information from the otolith organs facilitates correct perception of the orientation of the head with respect to gravity.
The otolith organs function so that any linear acceleration displaces the otoconial mass and applies a shear force on the embedded sensory hair bundles against the otolith maculae. This results in a potential change in the sensory cell and consequently a change in the discharge rate of the primary afferent vestibular nerve.
Since the earth’s gravity constitutes a constant linear acceleration, the orientation of the head relative to gravity is constantly signaled from the otolith organs to the central nervous system (Clarke, 2002). As a result, the individual can accurately estimate the so-called SVV.
Any dysfunction of the otolith apparatus is usually accompanied by incorrect spatial orientation and postural instability. The estimation of the SVV thus serves as a diagnostic indicator of otolith (utricular) function (Clarke et al, 2001).
How to perform the SVV test
The SVV is determined by presenting the patient with a luminous line in otherwise total darkness and requesting that they rotate the line to be in a perceived vertical alignment (Clarke et al, 2003). The test can be performed as either a static or dynamic protocol.
In the dynamic SVV test, the patient is spinning at 300 degrees per second, typically at 4 cm off axis to place the axis of rotation in line with the utricle. Centripetal acceleration applied to either the right or left labyrinth allows for independent utricular evaluation without influence from the other ear.
Once the patient has been rotating at a constant velocity for approximately one minute and the per-rotary nystagmus has subsided, the SVV trials are initiated.
It is possible to also perform static SVV tests without off axis centripetal acceleration. However, static SVV testing provides simultaneous stimulation of the otolith organs.
On the other hand, dynamic SVV testing completed during unilateral centripetal acceleration permits exclusive stimulation to the right or to the left utricle for improved specificity (Clarke et al, 2001) and enhances the diagnosis, particularly for peripheral vestibular disorders (Schonfeld & Clarke, 2011).
Numerous studies have documented that SVV may also be sensitive to central pathologies, such as brainstem or cerebellar lesions (Akin et al, 2011).
Findings in previous static SVV studies
For the static SVV, normal individuals can adjust the luminous line to within a few degrees of the gravitational vertical. Patients with unilateral otolith abnormalities will deflect the top of the line (SVV) toward the dysfunctional side.
However, patients with a compensated unilateral peripheral impairment will often have static SVV estimates that appear within normal limits. The published data shows ±2.0° as the normal tolerance (Akin & Murnane, 2009).
In the acute stage of a peripheral vestibular lesion such as vestibular neuritis, the static SVV shows an increase in deviation (>2°) toward the side of the lesion (Byun et al, 2010). The normal tolerance of ±2.0 does not change for on-axis rotation (Akin et al, 2011).
There is no gender effect and no significant change in static SVV with aging (Kobayashi et al, 2002).
Findings in previous dynamic SVV studies
The normal tolerance for off-axis dynamic SVV increases relative to the static test. As one may anticipate, normal individuals will present with larger SVV estimates as the axis of rotation deviates from center during unilateral centripetal acceleration.
Normal individuals will have SVV estimates tilted to the right during off-axis left dynamic testing and estimates tilted to the left during off-axis right dynamic testing (Akin et al, 2011). Akin et al reported off-axis rotation SVV angles as great as 11.0° for normal individuals, with normative values of –3.0° (SD=2.1°) for chair offset to the right, and 5.0° (SD=2.6°) for chair offset to the left.
Because of the variability within the normal population for dynamic off-axis SVV testing, the authors recommend using <11.0° as the cutoff value for normal and suggest that using a difference angle (on-axis value minus off-axis value) will reduce variability and bias when using the test for diagnostic purposes.
Concluding remarks on the use of the SVV test
The SVV test is recommended for acute vertigo, brainstem infarcts, and oculomotor disorders. The test can also be used to monitor recovery/compensation of acute lesions. It is considered a novel approach to assessment of otolith function that can be easily incorporated into the clinical test battery (Clarke et al, 2001).
References
Akin FW, Murnane OD. (2009) Subjective visual vertical test. Seminars in Hearing 30(4):281-286.
Akin FW, Murnane OD, Pearson A, Byrd S, Kelly JK. (2011) Normative data for the subjective visual vertical test during centrifugation. J Am Acad Audiol 22:460-468.
Byun JY, Hong SM, Yeo SG, Kim SH, Kim SW, Park MS. (2010) Role of subjective visual vertical test during eccentric rotation in the recovery phase of vestibular neuritis. Auris Nasus Larynx 37(5):565-569.
Clarke AH, Schönfeld U, Hamann C, Scherer H. (2001) Measuring unilateral otolith function via the otolith-ocular response and the subjective visual vertical. Acta Otolaryngol Suppl 545:84-87.
Clarke AH. (2002) The many facets of the otolith: a review. J Vestib Res 11(3-5):314.
Clarke AH, Schönfeld U, Helling K. (2003) Unilateral examination of utricle and saccule function. J Vestib Res 13:215–225.
Kobayashi H, Hayashi Y, Higashino K, Saito A, Kunihiro T, Kanzaki J, Goto F. (2002) Dynamic and static subjective visual vertical with aging. Auris Nasus Larynx 29(4):325-328.
Schoenfeld U, Clarke AH. (2011) A clinical study of the subjective visual vertical during unilateral centrifugation and static tilt. Acta Oto-Laryngologica 131: 1040-1050.
