
Short Increment Sensitivity Index (SISI) Test
Description
Table of contents
- What is the SISI test?
- Why SISI was developed
- When to consider SISI in a modern clinic
- How to perform the SISI test
- Results interpretation
- Diagnostic alternatives or additions
What is the SISI test?
The short increment sensitivity index (SISI) test is a behavioral audiometric measure which seeks to assess the listener’s ability to detect very small changes in stimulus intensity at suprathreshold levels. Clinically, the SISI test is used to assist with differentiating between cochlear and retrocochlear hearing loss (Lamoré & Rodenburg, 1980).
The core principles underlying the logic of the SISI test are:
- Cochlear hearing loss typically presents with abnormal loudness growth (recruitment).
- Retrocochlear hearing loss often presents with abnormalities in suprathreshold processing, without a typical loudness recruitment pattern.
By this logic, an individual with loudness recruitment (from a cochlear lesion) is more likely to detect very small suprathreshold changes in amplitude during the SISI test than a person with suprathreshold processing differences (from a retrocochlear lesion).
You can perform the SISI test using a range of Interacoustics audiometers, such as the Affinity Compact and Equinox Evo.
Why SISI was developed
Using the detection of small amplitude differences to assess loudness recruitment was first described in 1959 by Jerger and colleagues (Jerger et al., 1959). During this time, psychoacoustic measures were the primary means for site-of-lesion assessment in audiological medicine.
SISI was designed to be used alongside other tests (see Table 1) as part of a diagnostic battery aimed at differentiating cochlear from retrocochlear pathology based on patterns of loudness recruitment, auditory adaptation, and auditory fatigue. This was sometimes referred to as the “Special Audiometric Test Battery” (Clemis et al., 1976).
| Test |
| Acoustic reflex testing |
| Alternate binaural loudness balance (ABLB) |
| SISI |
| Speech testing |
| Tone decay testing |
Table 1: Diagnostic test battery for differentiating cochlear from retrocochlear pathology.
Before we move on to when and how to perform the SISI test, let’s consider loudness recruitment and cochlear gain in more detail. If you’d prefer to skip, please jump forward using the following links:
Loudness recruitment and cochlear gain
Loudness recruitment is a cochlear hearing loss, displayed by an abnormally rapid growth of perceived loudness with increasing level. This results in a reduction in the dynamic range of hearing (Shi et al., 2022). SISI is an intensity-discrimination task which is sensitive to these loudness-growth characteristics (Jerger et al., 1959; Schlauch & Wier, 1987).
Loudness recruitment is generally attributed to reduced cochlear amplification and loss of compressive non-linearity, which are changes commonly linked to outer hair cell dysfunction and an altered basilar membrane input-output function (Moore et al., 1999).
Recruitment differs from hyperacusis in that recruitment is usually linked to cochlear dysfunction, whereas hyperacusis is more commonly framed as a disorder of reduced sound tolerance with an important central component, often discussed in terms of altered central gain (Shi et al., 2022). However, it is important to recognize that these experiences are not necessarily mutually exclusive in clinical practice (Baguley, 2003; Paulin et al., 2016).
When to consider SISI in a modern clinic
Clinical indications for performing SISI as part of a diagnostic psychoacoustic test battery may include questions such as:
- “Is the patient’s hearing loss due to cochlear or retrocochlear pathology?”
- “Is the patient experiencing loudness recruitment?”
Answering these questions can have significant implications on the management decisions made as doing so may highlight the need for further medical investigations and/or changes to hearing aid provisions, such as considering amplification changes and/or provision of CROS or BAHA devices (Di Pasquale Fiasca et al., 2023).
Read more: CROS/BiCROS Hearing Aid Fitting
SISI and its accompanying test battery can be particularly useful in cases where you need behavioral confirmation of cochlear vs retrocochlear pathology, or cases where behavioral cross-checking is clinically valuable when objective measures are unavailable or inconclusive (Hoth & Baljić, 2017).
How to perform the SISI test
Below, we’ll cover the SISI test procedure step-by-step.
1. Establish the pure-tone threshold at the test frequency
SISI uses sensation level to determine stimulus presentation intensity. Before you start SISI, you therefore need to obtain a pure tone audiogram.
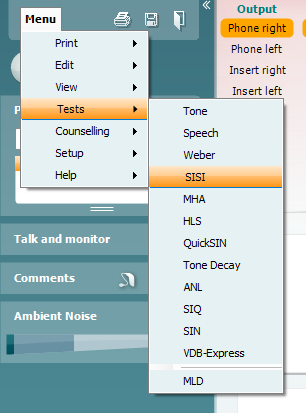
2. Open the “SISI” test protocol
If you are using an audiometer powered by the Affinity/Equinox Suite, navigate to the test selection menu in the top left and click on “SISI” (Figure 1).
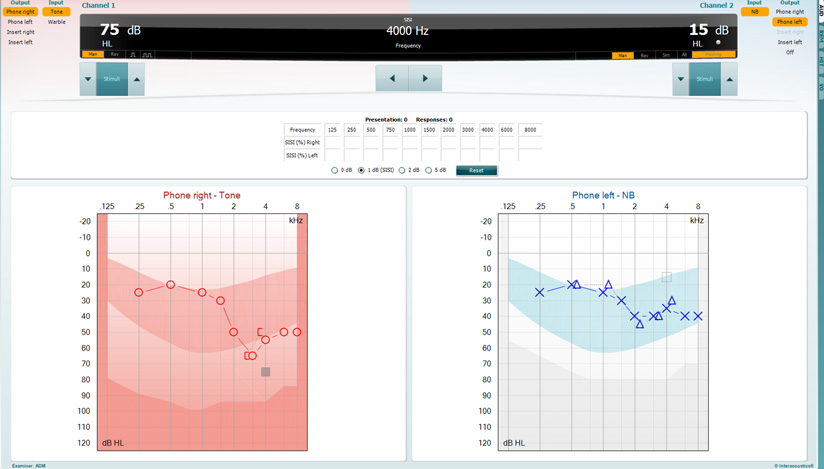
3. Select your transducer, starting frequency, and stimulus intensity
You should perform SISI with air conduction transducers. Thus, select the appropriate transducers for Channel 1 and select the test ear (Phone right/left). Use the arrow buttons to select the frequency you wish to test.
Next, using the recorded audiogram, use either your keyboard or on-screen buttons to select a presentation level of 20 dB sensation level (Figure 2).
4. Instruct your patient
An example of some simple instructions you could give to your patient are:
“You will hear a steady, constant tone. Sometimes the tone will get slightly louder for a moment. Each time you notice the brief increase in loudness, press the button.”
5. Training trials
It can be helpful to begin with an “easy” example by setting the pulse level to be 5 dB different. To change the level difference, use the check boxes below the results table. You should not use these training examples as a diagnostic trial, but to confirm understanding of the test.
6. Begin the test
To start, click on the “Start” button in the bottom left corner of the screen. This will start presenting the carrier tone and automatically present the higher intensity “pulses”. The most used protocol is a 1-dB increment, presented for 200 milliseconds with 20 total presentations.
7. Finishing and scoring the test
When testing with the Affinity/Equinox Suite, the test will automatically stop and record the score once 20 presentations have been delivered. You can stop the test early at any point by pressing the “Stop” button in the bottom left of the screen. Scoring is done by the audiometer automatically if 20 presentations were delivered and is given in percentage form for each tested frequency.
Results interpretation
The total percentage of identified intensity pulses is the primary outcome measure of the SISI test. Interpretation guidance varies slightly between sources, but generally falls around the ranges of:
| Percentage of identified intensity pulses | Interpretation |
| 0-20% | Normal hearing, conductive hearing loss, or retrocochlear hearing loss. |
| 20-70% | Inconclusive. |
| 70-100% | Consistent with cochlear pathology and associated recruitment. |
Table 2: Interpreting SISI test results (Jerger et al., 1959; Yantis & Decker, 1964).
While a high score is consistent with cochlear pathology, it is important to consider the wider clinical context such as the audiogram and any reported loudness intolerance. Low scores do not definitively rule out a cochlear pathology as although loudness recruitment is common in cochlear loss, it is not universal.
Finally, interpretation of the SISI test should always be part of a wider diagnostic assessment and you should never use it as the sole site-of-lesion assessment.
Diagnostic alternatives or additions
While behavioral measures such as the SISI test were historically central to site-of-lesion assessment, modern audiological diagnostics increasingly incorporate objective measures that provide direct information about cochlear and neural function. These procedures complement behavioral audiometry and allow clinicians to cross-check findings using objective physiological data (Hoth & Baljić, 2017).
For example, otoacoustic emissions (OAEs) provide a measure of cochlear outer hair cell function and are widely used to assess cochlear integrity and differentiate sensory from neural disorders (Kemp, 2002).
Auditory brainstem response (ABR) testing offers an objective assessment of neural conduction and synchrony within the auditory nerve and brainstem pathways, making it particularly useful when you suspect retrocochlear pathology (Eggermont, 2019).
Imaging studies (CT and MRI) have in recent decades become more central to the diagnostic process of many types of retrocochlear pathology such as acoustic neuroma (Kabashi et al., 2020).
These objective procedures have reduced reliance on behavioral site-of-lesion tests such as SISI in routine clinical diagnostics. Nevertheless, behavioral measures can still provide useful supplementary information about suprathreshold auditory processing and loudness growth when interpreted within the context of the wider test battery – particularly relating to loudness recruitment which is a largely perception phenomenon.
Summary
The SISI test is a behavioral measure of suprathreshold intensity discrimination, used to assess sensitivity to very small changes in sound level. It is particularly useful for identifying loudness recruitment, a characteristic feature of many cochlear hearing losses.
When interpreted alongside the audiogram and other clinical findings, SISI provides valuable insight into loudness growth and supports site-of-lesion assessment within a comprehensive test battery.
References
Baguley D. M. (2003). Hyperacusis. Journal of the Royal Society of Medicine, 96(12), 582–585.
British Society of Audiology. (2018). Recommended procedure: Pure-tone air-conduction and bone-conduction threshold audiometry with and without masking.
Clemis, J. D., & Mastricola, P. G. (1976). Special audiometric test battery in 121 proved acoustic tumors. Archives of otolaryngology (Chicago, Ill. : 1960), 102(11), 654–656.
Eggermont J. J. (2019). Auditory brainstem response. Handbook of clinical neurology, 160, 451–464.
Di Pasquale Fiasca, V. M., Sorrentino, F., Conti, M., De Lucia, G., Trevisi, P., de Filippis, C., Zanoletti, E., & Brotto, D. (2023). Hearing Aid in Vestibular-Schwannoma-Related Hearing Loss: A Review. Audiology research, 13(4), 627–635.
Hoth, S., & Baljić, I. (2017). Current audiological diagnostics. GMS current topics in otorhinolaryngology, head and neck surgery, 16, Doc09.
JERGER, J., SHEDD, J. L., & HARFORD, E. (1959). On the detection of extremely small changes in sound intensity. A.M.A. archives of otolaryngology, 69(2), 200–211.
Kabashi, S., Ugurel, M. S., Dedushi, K., & Mucaj, S. (2020). The Role of Magnetic Resonance Imaging (MRI) in Diagnostics of Acoustic Schwannoma. Acta informatica medica : AIM : journal of the Society for Medical Informatics of Bosnia & Herzegovina : casopis Drustva za medicinsku informatiku BiH, 28(4), 287–291.
Kemp D. T. (2002). Otoacoustic emissions, their origin in cochlear function, and use. British medical bulletin, 63, 223–241.
Lamoré, J. J., & Rodenburg, M. (1980). Significance of the SISI test and its relation to recruitment. Audiology : official organ of the International Society of Audiology, 19(1), 75–85.
Moore, B. C., Glasberg, B. R., & Vickers, D. A. (1999). Further evaluation of a model of loudness perception applied to cochlear hearing loss. The Journal of the Acoustical Society of America, 106(2), 898–907.
Paulin, J., Andersson, L., & Nordin, S. (2016). Characteristics of hyperacusis in the general population. Noise & health, 18(83), 178–184.
Schlauch, R. S., & Wier, C. C. (1987). A method for relating loudness-matching and intensity-discrimination data. Journal of speech and hearing research, 30(1), 13–20.
Shi, L., Zhao, R., Li, X., Sun, W., & Liu, X. (2022). A Review of the Neurobiological Mechanisms that Distinguish Between Loudness Recruitment and Hyperacusis. Medical science monitor : international medical journal of experimental and clinical research, 28, e936373.
YANTIS, P. A., & DECKER, R. L. (1964). ON THE SHORT INCREMENT SENSITIVITY INDEX (SISI TEST). The Journal of speech and hearing disorders, 29, 231–246.
Presenter
