
Masking Level Difference (MLD)
Description
Table of contents
What is the MLD test?
The Masking Level Difference (MLD) test is a psychoacoustic measure of binaural interaction (de Carvalho et al., 2021). In other words, it assesses the auditory system’s ability to integrate signals presented to both ears.
The MLD test is particularly sensitive to abnormalities within the lower auditory brainstem, where interaural time differences (ITDs) are encoded. For this reason, it is commonly used in the evaluation of brainstem integrity and auditory processing function.
Because the task does not rely on language, the MLD has become a valuable clinical tool for assessing auditory processing disorders (APD), particularly in cases where binaural temporal processing deficits are suspected.
Theoretical background
The MLD test measures an individual’s ability to detect tonal signals in the presence of masking noise. During the procedure, the phase of either the signal or the masking noise is systematically inverted.
The underlying psychoacoustic principle is that when the signal and noise are presented in-phase (homophasic condition), detecting the signal is more difficult. Whereas detection improves when the signal and noise are out of phase (antiphasic condition).
This improvement occurs because in the antiphasic condition the two waveforms differ in both their temporal and amplitude characteristics, allowing the auditory system to exploit binaural cues to achieve a release from masking (Cekic et al., 2024; Olsen et al., 1976).
Masking configurations
The test typically uses two (plus an optional third) masking configurations.
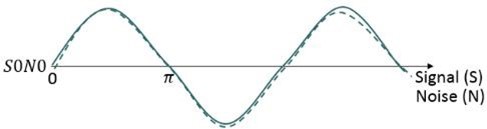
Step 1: Measure S₀N₀, where the signal and noise are in phase at both ears. This step is compulsory.
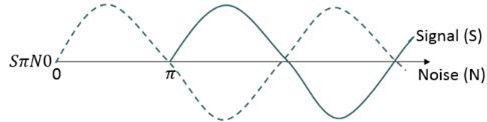
Step 2: Measure the SπN₀, where the signal is phase‑reversed by 180 degrees between ears. This step is also compulsory.
Optional step 3: Measure the S₀ SπN₀, where the noise is phase‑reversed by 180 degrees between ears.
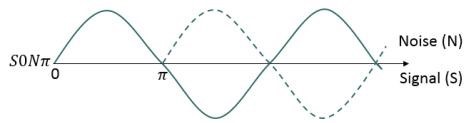
The MLD is defined as the improvement in the masked threshold for a tone when the phase of either the signal or the masking noise is inverted by 180 degrees in one ear. The largest MLD is typically observed in SπN₀, because reversing the signal phase exploits binaural timing cues while keeping the masker aligned across ears (Noffsinger et al., 1984).
MLD test procedure
Given its clinical applications, the MLD test is mainly performed in individuals with normal hearing as measured by pure tone audiometry. To complete an MLD test, you need a 2-channel audiometer. The following clinical audiometers from Interacoustics can complete the MLD test: Equinox Evo and AC40.
The test comprises of nine simple steps.
1. Provide patient instructions
Before beginning the test, instruct the patient clearly to ensure accurate behavioral responses:
“In this test, you will hear a steady noise in both ears along with some very soft beeping tones. Your task is to press the button whenever you hear the tone and release the button as soon as the tone disappears. The loudness and the way the sounds are presented may change during the test, but your task remains the same throughout. Press when you hear the tone and release when it stops.”
2. Select and position the transducer
Choose the desired transducer for the test: Insert earphones, circumaural headphones, or supra‑aural headphones. Perform otoscopy before transducer positioning and check correct placement and a proper acoustic seal.
3. Select the test frequency
MLD effects are largest at low frequencies. Therefore, the test is typically performed at 250 or the most used 500 Hz. Only one frequency is required, but you can test more depending on your clinical goals. 125 and 750 Hz are also optional to test.
4. Set the initial stimulus intensity
The test always starts with the homophasic (S₀N₀) condition: Present the narrowband noise at a fixed level, typically 60 dB HL in both ears. The tone level is adjustable and will be modified during threshold seeking.
5. Set the step size
Use a 2-dB step size. Standard 5-dB steps are too large and reduce precision for MLD threshold comparisons.
6. Measure the S₀N₀ (homophasic) condition
Begin the test by presenting the tone and noise in phase at both ears. The noise remains fixed; the clinician adjusts the tone. Use the standard ascending‑threshold procedure to determine the tone threshold within the masking noise. Store the masked threshold for this condition.
7. Measure the SπN₀ (antiphasic) condition
Reverse the phase of the signal by 180 degrees in one ear by selecting the SπN₀ condition on the audiometer. Keep the noise identical to the previous condition (in phase across ears). Begin again at 60 dB HL and adjust the tone to find threshold. Store the masked threshold.
8. Measure the S₀Nπ condition (optional)
This condition reverses the phase of the noise, not the signal. If performed, repeat the same threshold‑seeking procedure. Store the masked threshold.
9. Calculate the MLD
The MLD is calculated by subtracting the masked threshold for the antiphasic condition (see step 7) from the masked threshold for the homophasic condition (see step 6).
Most modern audiometers including the Equinox Evo and AC40 from Interacoustics will calculate this automatically. The example below shows how to calculate the MLD if you do not have one of these devices.
Example calculation
If the masked threshold in S₀N₀ is 60 dB, and reversing the signal phase (SπN₀) gives a threshold of 44 dB, then the MLD is 16 dB (60 minus 44).
MLD results interpretation
You can compare the final MLD value against published normative data to determine whether binaural interaction is within normal limits. Musiek (2013) recommends the following levels when calculating the MLD based on the equation: S₀N₀ minus SπN₀ (Table 1).
| MLD value | Interpretation |
| 10 dB or more | Normal binaural unmasking |
| 7 to 9 dB | Borderline; interpret with caution |
| 6 dB or less | Abnormal; suggests impaired binaural processing |
Table 1: Interpreting MLD values.
Cekic et al. (2024) report similar results in their paper with an MLD mean of 10.3 ± 1.99 dB for the S₀N₀ minus SπN₀ condition. They also provide an MLD mean for the S₀N₀ minus S₀Nπ condition of 6.72 ± 2.38 dB. Remember, the most used MLD calculation is the S₀N₀ minus SπN₀ condition.
If you record an abnormally small MLD, this suggests atypical binaural interaction. You should then perform the following steps before further interpretations:
- Confirm peripheral hearing and rule out conductive components.
- Consider adding S₀Nπ for further diagnostic insight.
- Interpret results alongside a broader test battery (dichotic tests, temporal processing, ABR, speech-in-noise).
Conclusion
The MLD is a valuable, time-efficient measure of binaural interaction with high clinical utility. Its strength lies in understanding brainstem timing mechanisms using low-frequency stimuli where ITDs dominate.
References
Brown, M., & Musiek, F. (2013). The fundamentals of masking level differences for assessing auditory function. Hearing Journal, 66(1), 16-17.
Cekic, S., Mujdeci, B., Karakoc, K., & Bas, B. (2024). Masking level differences under two different measurement conditions: A normative study of young adults. Brain and Behavior, 14(9), e370011.
de Carvalho, N. G., Amaral, M., de Barros, V. Z., & Santos, M. (2021). Masking level difference: Performance of school children aged 7–12 years. Journal of Audiology & Otology, 25(2), 65–71.
Noffsinger, D., Schaefer, A. B., & Martinez, C. D. (Eds.). (1984). Behavioral and objective estimates of auditory brainstem integrity. Seminars in Hearing. Thieme Medical Publishers.
Olsen, W. O., & Noffsinger, D. (1976). Masking level differences for cochlear and brainstem lesions. Annals of Otology, Rhinology & Laryngology, 85(6), 820–825.
Presenter
