
cVEMP Testing
What is the cervical vestibular evoked myogenic potential (cVEMP)?
The cervical Vestibular Evoked Myogenic Potential (cVEMP) is an evoked potential measured from the sternocleidomastoid (SCM) muscle and is used to assess the vestibular system (the saccule and its afferent pathways). An amplitude asymmetry ratio is then calculated to assess if the vestibular system is working normally. VEMP tracings are easily recorded and provide valuable information to medical practitioners to assist them in the diagnosis of various disorders. Loud tone bursts, at slow rates are used to elicit this response. 
Why cVEMP?
The cVEMP is a test used in addition to traditional vestibular testing (e.g., VNG) to assist in the assessment of vestibular function. The cVEMP provides information about the saccule and inferior vestibular nerve, assisting medical practitioners in the diagnosis of disorders such as Superior Semicircular Canal Dehiscence (SSCD) (Milojcic et al., 2013) and Meniere’s disease (Rauch et al., 2004).
How to test?
Patient preparation
The electrode sites must be prepared and cleaned in order to obtain acceptably low skin impedances. It is recommended to have impedance values of 3kΩ or lower. The impedance values between each electrode should be balanced or similar in value.
There are different suggested activation techniques for the SCM muscle. The patient can either be sitting and instructed to turn the head only to contract/activate the SCM muscle as shown in the image below. Alternatively, the patient can be in a reclined position and asked to lift the head and turn the neck to contract the SCM muscle. Use of the patient EMG monitor will ensure consistent activation during testing.
Electrode placement (example)

The reference electrodes should be placed on the upper belly of the SCM muscle on both sides. The vertex electrode is placed on the clavicular joint (or on the high forehead) and the ground/common on the low forehead.
Typically, the air-conduction stimulus used is a 500Hz tone burst at high intensity level (e.g., 90/95dBnHL).
Ensure that the patient is relaxed prior to starting the test. After confirming impedances.
Setting up the Eclipse
The Eclipse comes with pre-programmed cVEMP protocols so the system is ready to use immediately. Protocols can be created or modified easily to fit your clinical needs. Consult the Eclipse Additional Information document to learn how to create or modify a protocol. The procedure described below is simply a suggested test process and to be used only as a guideline.
Patient monitor
An adequate contraction of the SCM muscle is essential for a good cVEMP recording. The patient monitor provides information to the patient during testing to ensure a correct head turn/lift and informs the patient about the test time and contraction of the SCM muscle. The information provided on the patient monitor is a guide to the patient and constitutes to a more accurate test procedure which may shorten the overall test time.

EMG controlled stimulus/recording
EMG controlled stimulus/recording means the system will only collect data when the patient contracts the SCM muscle adequately. This can be monitored by the patient either visually Patient EMG Monitor or audibly Monitor Tone. Please see Additional Information document for a more detailed explanation of monitoring options.

cVEMP testing procedure
Choose a cVEMP protocol from the dropdown menu 
The cVEMP test should be run in the Manual Mode controlling/selecting stimuli manually.
Manual mode
- To begin in manual mode, choose the intensity and select the ear to test on the Record sheet. Instruct the patient to turn their head to the right or left to activate the muscle on the testing side. You should pay particular attention to the ongoing EEG and the target range if needed.
- Next choose Start or hit F2.
- 100-200 sweeps are typically collected per waveform.
Setting up L & R waveform partners
After collection, choose a left or right ear waveform by double clicking the waveform handle. Next, right click the waveform handle of the opposite ear and select Set as VEMP Partner. The selected waveforms are used in the Asymmetry Ratio Calculation.
EMG scaling
The default protocol is setup to scale the curves automatically. Some prefer to scale after the recordings are completed. After the recording is complete, you can right click on the waveform and choose EMG Scaling. Waveforms will then be scaled according to the average pre-stimulus EMG values recorded throughout the collection. This will make individual recordings comparable, even though slightly different degrees of muscle tonus may have been applied during the different recordings, which provides a reliable tool in calculation of the amplitude asymmetry (McCaslin et al., 2014).
HINT Display Scaling can be increased or decreased by using the arrows on the top left side of the recording window or by using your keyboard arrows
Marking peaks
The cVEMP response is well documented and is said to be represented by two distinct peaks; P1 occurring at approximately 13 ms and N1 occurring at approximately 23 ms.
Waveforms can be marked from the Record sheet or the Edit sheet. To mark a waveform double click on the waveform handle you would like to mark. Right click and then choose the correct marker. Drag your mouse to the correct area and click. You can also choose 1-4 on the keyboard to bring up the appropriate marker and use Enter to place it.
Normative data
A number of studies report upper limits of normal for cVEMP recordings between 35 – 45% depending on the use of EMG monitoring and scaling of the response. In a study by McCaslin and colleagues (2013), the upper limit of normal was reported as ~31-37 % when both EMG monitoring and scaling was applied.
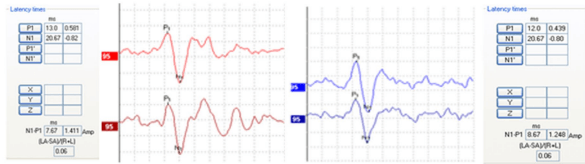
Example of a cVEMP where P1 and N1 are marked for both ears. The asymmetry ratio is calculated at 0.06. Curves are scaled.

Example of scaled cVEMP waveforms indicating an abnormal asymmetry ratio (0.80) between left and right side, along with lowered cVEMP thresholds on the right. (Curves in the above example are inverted).
Reporting
Choose the Report Icon ![]()
When complete, choose Save and Exit.
References
McCaslin, D. L., Fowler, A., Jacobson, G. P. (2014). Amplitude normalization reduces cervical vestibular evoked myogenic potential (cVEMP) amplitude asymmetries in normal subjects: proof of concept. J Am Acad Audiol, 25(3), 268-277.
McCaslin, D. L., Jacobson, G. P., Hatton, K., Fowler, A. P., & DeLong, A. P. (2013). The effects of amplitude normalization and EMG targets on cVEMP interaural amplitude asymmetry. Ear Hear, 34(4), 482-490.
Milojcic, R., Guinan, J.J., Rauch, S.D., & Herrmann, B.S. (2013). Vestibular evoked myogenic potentials in patients with superior semicircular canal dehiscence. Otol Neurotol, 34(2), 360-367.
Rauch, S. D., Zhou, G., Kujawa, S. G., Guinan, J. J., Herrmann, B. S. (2004). Vestibular evoked myogenic potentials show altered tuning in patients with Ménière’s disease. Otology & Neurotology, 25(3), 333-338.
Young, Y. H., Wu, C. C., & Wu, C. H. (2002). Augmentation of vestibular evoked myogenic potentials: an indication for distended saccular hydrops. Laryngoscope, 112(3), 509-512